As the American healthcare landscape faces the dual pressures of skyrocketing premiums and a shifting regulatory environment, a significant legislative trend is emerging at the state level: the introduction of targeted tax credits designed to incentivize the adoption of Health Reimbursement Arrangements (HRAs). This movement, spearheaded by Indiana and rapidly gaining momentum in states like Connecticut and Mississippi, represents a fundamental shift in how state governments support small and mid-sized businesses. By offering fiscal relief to employers who pivot from traditional group health insurance to individual coverage models, lawmakers are attempting to stabilize the small-group market while providing employees with greater autonomy over their healthcare choices.
The Shift Toward Defined Contribution Healthcare
For decades, the "defined benefit" model—traditional group health insurance—has been the standard for American employment. Under this model, employers select a specific plan and cover a portion of the premium, leaving employees with limited choices and employers with unpredictable annual cost increases. However, the emergence of the Individual Coverage HRA (ICHRA) and the Qualified Small Employer HRA (QSEHRA) has introduced a "defined contribution" alternative.
Under an HRA, employers provide a tax-free allowance that employees use to purchase their own health insurance on the individual market. This allows businesses to control their budgets with precision while decoupling the employment relationship from a specific insurance carrier. Recent data from the HRA Council underscores the rapid adoption of these models, noting a 19% year-over-year increase in combined ICHRA and QSEHRA adoption between 2024 and 2025. ICHRAs, in particular, have seen a 21% surge, driven by their lack of contribution limits and their availability to businesses of all sizes.
Indiana: The Architect of the HRA Tax Credit
The current wave of state-level incentives can be traced back to Indiana’s House Bill 1004. Enacted in 2024, the legislation established Indiana as the first state to provide a direct tax credit for small employers—those with fewer than 50 employees—who replace their traditional group plans with an HRA.
The Indiana model is structured to provide immediate relief during the critical transition period. In the first year of implementation, employers receive a tax credit of up to $400 per covered employee. This credit continues into the second year at a rate of up to $200 per employee. The logic behind this two-year "runway" is to mitigate the administrative and psychological hurdles associated with moving away from the familiar, if flawed, group insurance system. By reducing the net cost of the benefit in the early stages, Indiana lawmakers successfully lowered the barrier to entry for hundreds of small businesses that previously felt priced out of the benefits market.
A Growing Legislative Map: 2025-2026 Developments
Following Indiana’s lead, several states moved to introduce similar legislation during the 2025 and 2026 sessions. The results have been a mix of successful enactments and exploratory bills that signal a bipartisan interest in healthcare affordability.
Connecticut’s High-Stakes Incentive
In 2026, Connecticut approved Public Act 26-68 as part of its annual budget. The state’s approach is notably more aggressive than Indiana’s, offering a match of employer contributions up to $1,000 per covered employee per year for the first two years. With a total program cap of $5 million, Connecticut is positioning itself as a laboratory for high-incentive HRA adoption, specifically targeting the ICHRA model to bolster its state insurance exchange.
Mississippi’s Direct Replication
Mississippi joined the movement in 2026, enacting a tax credit that mirrors the Indiana structure: $400 per employee in the first year and $200 in the second. Mississippi legislators cited the need to support the state’s rural small businesses, many of which have struggled to maintain group coverage as providers exit the small-group market.
The Proliferation of Proposed Legislation
While not all bills have crossed the finish line, the volume of activity is unprecedented:

- Ohio: Introduced an ICHRA tax credit of $400 per employee in 2025. While it passed the House, it remains under deliberation in the Senate.
- Georgia: Proposed a multi-year sliding scale credit starting at $600 per employee for the first three years, dropping to $200 by the fifth year. This long-term commitment aims to ensure sustained participation.
- Illinois and New Hampshire: Both states introduced bills in 2026 (SB 3619 and SB 635, respectively) targeting $400 per employee credits. New Hampshire’s proposal includes a $10 million total cap, reflecting a cautious but optimistic fiscal approach.
Economic Drivers: Why Now?
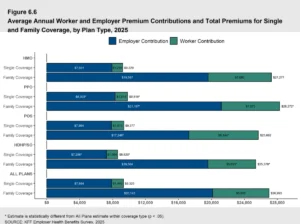
The legislative push for HRA tax credits is a direct response to a widening gap in the American benefits system. According to data from KFF, there is a stark disparity in healthcare offering rates based on company size. While 97% of organizations with 200 or more workers offer health benefits, that number plummets to just 59% for businesses with 10 to 199 workers.
The primary culprit is cost volatility. Group health insurance premiums have historically risen at rates that significantly outpace inflation. For a small business with thin margins, a 15% annual premium hike can be the difference between profitability and loss. HRAs solve this by allowing the employer to set a fixed "contribution" (e.g., $500 per month per employee). If insurance prices rise, the employer’s cost remains stable unless they choose to increase the allowance.
States have a vested interest in this shift. When small businesses drop coverage, their employees often end up uninsured or relying on state-subsidized programs. By incentivizing HRAs, states are essentially shoring up the individual market. More HRA participants mean a larger, more diverse risk pool in the individual exchanges, which can lead to more competitive pricing and more carrier options for all residents.
Overcoming the "Risk of Change"
Despite the clear financial advantages, many employers remain hesitant to abandon the traditional group insurance model. This hesitation is often rooted in "the devil you know" syndrome—the fear that employees will find the individual market too complex or that the transition will create an administrative burden.
State tax credits serve as a powerful "nudge." They provide a financial cushion that allows human resources departments to invest in education and transition support. Furthermore, the rise of HRA administration platforms, such as PeopleKeep and Remodel Health, has automated the compliance and reimbursement aspects of these plans, removing the operational barriers that once made HRAs a niche product.
Analysis of Implications for the Healthcare Market
The widespread adoption of HRA tax credits could trigger several long-term market shifts:
- Individual Market Strengthening: As thousands of employees move from group plans to individual plans funded by their employers, the individual market gains a influx of "preferred risk" individuals—generally younger, healthier workers who were previously on group plans. This can stabilize premiums for everyone in the exchange.
- Increased Portability: One of the greatest flaws of the American healthcare system is "job lock," where employees stay in roles they dislike simply to keep their health insurance. HRAs promote portability; if an employee leaves a job, they keep their individual insurance policy, though they must find a new way to pay the premium.
- Broker Evolution: The traditional insurance broker model is being forced to evolve. Instead of simply negotiating a single group plan, brokers are increasingly becoming "benefit consultants" who help employers set up HRA structures and help employees navigate individual plan selections.
Looking Ahead: The 2027 Horizon
The next major milestone in this trend will occur in 2027, when Arizona is scheduled to release a comprehensive report on its study of ICHRA expansion for state and public school district employees. If a state as large as Arizona moves toward an HRA model for public sector workers, it could provide the ultimate proof of concept, potentially leading to a federal-level discussion on HRA incentives.
As of May 2026, the momentum is undeniable. With Indiana, Connecticut, and Mississippi leading the way, the tax credit model is proving to be a viable policy tool for states looking to protect small businesses from the "premium spiral." For employers, the message from state capitals is clear: the era of the one-size-fits-all group plan is ending, and a more flexible, tax-advantaged future is being built in its place.
In conclusion, the convergence of rising group costs, legislative innovation, and administrative technology has created a "perfect storm" for HRA adoption. While Indiana House Bill 1004 was the spark, the resulting fire is now spreading across the country, offering a rare example of a healthcare policy that aligns the interests of state treasuries, business owners, and individual employees alike. As more states evaluate the success of these early adopters, the HRA tax credit may soon move from a "trend" to a standard component of state economic development strategies.