The financial landscape for nonprofit organizations has reached a critical juncture as the cost of traditional employer-sponsored health insurance continues to outpace inflation and revenue growth. As of early 2026, the struggle to balance mission-driven objectives with the necessity of providing competitive employee benefits has intensified. For many small to mid-sized nonprofits, the rising tide of health insurance premiums has made traditional group healthcare coverage an unsustainable burden. In response, a growing number of organizations are pivoting toward the Qualified Small Employer Health Reimbursement Arrangement (QSEHRA) as a strategic alternative to the conventional group plan model.
The Economic Context of Rising Healthcare Costs
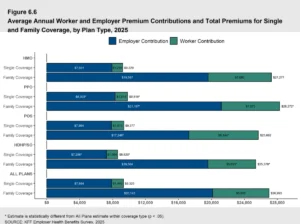
The shift toward reimbursement models is driven by stark economic realities. Data from the Kaiser Family Foundation (KFF) indicates that by 2025, the average annual premium for employer-sponsored health insurance reached approximately $9,325 for single coverage and $26,993 for family coverage. This represented a 5% increase in single premiums and a 6% increase in family premiums over the previous year. However, for small organizations—particularly those with high claims volume or employees managing chronic conditions—these averages often fail to tell the full story. Many such groups have reported "renewal shock," with premium hikes ranging from 20% to 30% in a single year.
For a 501(c)(3) organization operating on fixed grants or donor contributions, a 30% spike in a fixed cost like health insurance can necessitate cuts in programming or staffing. This volatility has led HR directors and CFOs in the nonprofit sector to seek "defined contribution" models, where the employer can set a fixed, predictable budget for health benefits, rather than being at the mercy of "defined benefit" group plans where the costs are dictated by insurance carriers.
The Regulatory Framework: A Brief History of the QSEHRA
The QSEHRA did not emerge in a vacuum. Its origins can be traced back to the 21st Century Cures Act, signed into law in December 2016. This bipartisan legislation was designed to provide relief to small businesses that had been prohibited from using stand-alone HRAs to help employees pay for individual health insurance following the implementation of certain Affordable Care Act (ACA) market reforms.
The QSEHRA framework was further bolstered by the Coronavirus Aid, Relief, and Economic Security (CARES) Act in 2020, which expanded the list of eligible medical expenses to include over-the-counter medications and menstrual care products without a prescription. These legislative milestones have solidified the QSEHRA as a permanent fixture in the IRS code, providing a stable foundation for nonprofits to build their benefits packages.
Mechanics of the QSEHRA for Small Nonprofits
The QSEHRA is specifically designed for employers with fewer than 50 full-time equivalent (FTE) employees who do not offer a group health insurance plan. Unlike traditional insurance, where the employer selects a plan and pays a portion of the premium to a carrier, the QSEHRA operates on a reimbursement basis.
Under this arrangement, the nonprofit establishes a monthly allowance for its employees. Employees then purchase their own individual health insurance policies on the open market or through the Health Insurance Marketplace. After providing proof of coverage and incurring eligible medical expenses—which can include premiums, deductibles, copayments, and even dental or vision care as outlined in IRS Publication 502—the employee submits a claim to the employer. The employer then reimburses the employee up to the limit of their allowance.
Financial Predictability and Budgetary Control
The primary advantage cited by nonprofit financial officers is the ability to control costs. In a QSEHRA, the employer decides exactly how much they can afford to contribute. There is no minimum contribution requirement, though the IRS does set annual maximum limits to ensure the benefit remains targeted at small employers.
Furthermore, the QSEHRA offers a "use-it-or-lose-it" benefit to the employer’s bottom line. If an employee does not utilize their full allowance within the plan year, the unused funds remain with the nonprofit. This is a significant departure from group plans, where premiums are paid regardless of whether the employee utilizes the medical services. For organizations where every dollar is earmarked for community impact, this efficiency is a major draw.
Tax Advantages and Compliance Requirements
From a tax perspective, the QSEHRA is highly efficient. When administered correctly, reimbursements made through a QSEHRA are 100% tax-free for both the employer and the employee. This means the nonprofit does not pay payroll taxes (FICA/FUTA) on the reimbursed amounts, and employees do not report the reimbursements as taxable income on their W-2s.
However, compliance is critical. To qualify for tax-free status, employees must maintain "minimum essential coverage" (MEC). If a nonprofit mistakenly reimburses an employee who does not have a qualifying health insurance policy, the IRS requires that the reimbursed amount be treated as taxable income. This necessitates rigorous documentation and administrative oversight, often managed through third-party platforms to ensure adherence to IRS and Department of Labor (DOL) regulations.

Empowering the Modern Nonprofit Workforce
The shift to a QSEHRA also reflects changing employee expectations. A 2024 Employee Benefits Survey conducted by PeopleKeep by Remodel Health revealed that 92% of employees consider health benefits a top priority when choosing or staying with an employer. However, the "one-size-fits-all" approach of traditional group plans is increasingly viewed as a drawback.
In a group plan, a young, healthy employee might be forced into a high-premium plan with benefits they don’t need, while an older employee might find the network of doctors too restrictive. By utilizing a QSEHRA, employees are empowered to shop for a plan that fits their specific needs, whether that is a plan with a specific provider network, a lower deductible, or a specialized prescription drug formulary. This personalization often leads to higher perceived value of the benefit, even if the dollar amount remains the same as what the employer would have contributed to a group plan.
Critical Considerations: The Premium Tax Credit Interaction
One of the most complex aspects of implementing a QSEHRA within the nonprofit sector is the interaction with government premium tax credits (PTCs). Many employees in the nonprofit sector, particularly those at lower income levels, may already be eligible for federal subsidies to help pay for Marketplace insurance.
According to IRS Code Section 36B, employees must coordinate their QSEHRA allowance with any PTCs they receive. If the QSEHRA allowance is deemed "affordable" by IRS standards, the employee must waive their premium tax credit entirely. If the allowance is "unaffordable," the employee can still claim the PTC, but they must reduce the amount of the credit dollar-for-dollar by the amount of the QSEHRA allowance.
For example, if an employee is eligible for a $500 monthly premium tax credit and their nonprofit employer offers a $200 monthly QSEHRA allowance, the employee’s available tax credit would be reduced to $300. Nonprofit leaders must proactively educate their staff on these nuances to avoid "benefit surprises" during tax season.
Comparing the QSEHRA and the ICHRA
While the QSEHRA is a popular choice for small nonprofits, it is not the only reimbursement model available. The Individual Coverage HRA (ICHRA), introduced in 2020, offers an alternative for organizations that may exceed the 50-FTE limit or require more flexibility.
Unlike the QSEHRA, the ICHRA has no maximum contribution limits and no employer size restrictions. Perhaps most importantly for larger nonprofits, the ICHRA allows for "classing." An organization could, for instance, offer a traditional group plan to full-time employees while offering an ICHRA to part-time or seasonal staff. This level of segmentation is not permitted under QSEHRA rules, which generally require that the benefit be offered on the same terms to all eligible employees.
Data Analysis: Benchmarking Monthly Allowances
Data from the 2025 QSEHRA Report provides a benchmark for nonprofits looking to remain competitive. On average, small employers offered a monthly allowance of $442 per employee. Interestingly, the data suggests that the smallest organizations often offer the most generous allowances:
- 1 to 4 Employees: $465 average monthly allowance
- 5 to 9 Employees: $444 average monthly allowance
- 10 to 19 Employees: $424 average monthly allowance
- 20 to 49 Employees: $415 average monthly allowance
These figures suggest that smaller nonprofits are leveraging the QSEHRA not just as a cost-saving measure, but as a robust tool to compete with larger corporations for top-tier talent.
Broader Implications for the Nonprofit Sector
The trend toward QSEHRAs represents a fundamental shift in the social contract between nonprofit employers and their staff. By moving away from the role of "insurance purchaser" and toward the role of "benefit facilitator," nonprofits are acknowledging the diversity of their workforce’s needs.
Industry analysts suggest that this shift could lead to a more resilient nonprofit sector. By decoupling health benefits from the volatile group insurance market, organizations can achieve greater long-term financial stability. This, in turn, ensures that more resources remain directed toward their core missions—whether that be social services, environmental advocacy, or the arts—rather than being absorbed by escalating administrative and insurance costs.
In conclusion, while the traditional group health insurance model remains a staple for many, the QSEHRA has emerged as a vital lifeline for small nonprofits. It offers a unique blend of tax efficiency, budgetary control, and employee choice that is uniquely suited to the constraints and values of the nonprofit world. As the healthcare market continues to evolve toward 2030, the adoption of flexible, reimbursement-based benefits is likely to become the new standard for mission-driven organizations across the United States.