The escalating cost of employee healthcare is no longer a looming threat; it is a present-day crisis actively undermining the financial health and operational capacity of American businesses. This assertion, far from hyperbole, is grounded in stark financial realities. Since 2001, the average annual premium for family healthcare coverage has surged dramatically, from approximately $7,100 to nearly $27,000. Even single coverage plans have more than tripled in cost. The magnitude of this financial burden is so profound that major corporations now report spending more on employee healthcare than on core operational expenses. For instance, Starbucks dedicates more resources to healthcare than to its namesake coffee beans, and the automotive industry finds itself allocating greater funds to employee health benefits than to steel, a fundamental component of vehicle manufacturing.
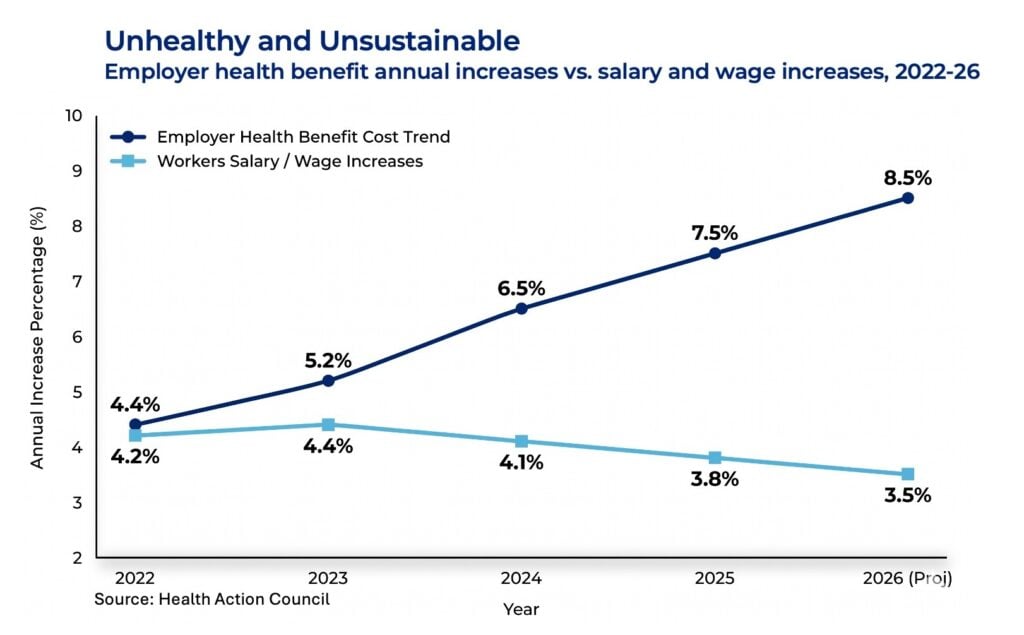
This trend is not merely continuing; it is accelerating. Projections for 2026 indicate an anticipated increase in healthcare spending ranging from 8.5 to 9.5 percent, a rate not seen in approximately 15 years. This unchecked rise in healthcare expenditures exerts significant pressure on several critical business functions, including wage growth, hiring capacity, pricing strategies, and ultimately, profit margins. For a substantial number of companies, the relentless climb of healthcare costs poses a direct impediment to investing in future growth and innovation.
Patty Starr, President and CEO of the Health Action Council, a coalition representing 240 employers, union groups, and nonprofits dedicated to improving employee health and cost containment, has been a frontline observer of this unfolding crisis for years. Her extensive experience has provided her with deep insights into the root causes of these escalating expenses and actionable strategies for employers to combat them.
"While we cannot resolve a crisis that has been decades in the making within a single year," Starr stated during a recent Chief Executive online presentation, "we can fundamentally shift our mindset and manage healthcare costs with the same business discipline we apply to other significant expenditures, thereby influencing specific areas of impact."
The Critical Blind Spot: Focusing on the Wrong Costs
Starr identifies a pervasive "blind spot" in how many organizations approach healthcare cost management. The common practice involves expending considerable energy and resources on scrutinizing fixed costs. These include administrative fees, stop-loss premiums, and broker and consultant fees. These expenses are easily quantifiable, appear clearly on spreadsheets, and are relatively straightforward to compare and negotiate. The perceived "wins" in reducing these line items can create a false sense of control and accomplishment.
However, this focus is fundamentally misplaced. Starr emphasizes that these fixed costs represent only a fraction of a company’s total healthcare spending, often accounting for no more than 20 to 25 percent. The vast majority of healthcare expenditures—estimated to be between 75 and 80 percent—lie within variable costs. These include the actual claims paid, service model expenses, network access fees, payment integrity fees, and crucially, the rapidly escalating costs associated with specialty pharmaceuticals. The problem, Starr argues, is that most organizations dedicate minimal attention and strategic effort to managing these variable costs.
"We may win the battle of the administrative fee spreadsheet," Starr observed, "but we ultimately lose significantly on our P&L because we are not addressing the true drivers of cost."
A Five-Point Action Plan to Tackle Variable Costs
To effectively address the escalating healthcare cost crisis, Starr proposes a comprehensive five-point action plan designed to provide employers with practical, actionable steps to regain control over this critical P&L item.

1. Cultivating Visibility and Control Through Data Analytics
"You cannot effectively manage what you cannot see or do not fully understand," Starr asserted. For self-insured employers, de-identified claims data should serve as the foundational element for strategic decision-making, rather than merely being presented as a retrospective analysis during renewal negotiations. Employers with fully insured plans, particularly those with over 100 employees, possess the leverage to demand more meaningful reporting from their carriers. This reporting should encompass detailed insights into health conditions, utilization patterns, site-of-care preferences, and geographical variations in healthcare delivery.
At a minimum, employers require access to medical and pharmacy claims data, eligibility information, location-specific utilization, detailed profiles of high-cost claimants, patterns of care delivery, vendor performance metrics, and employee engagement survey results. This level of visibility is essential for formulating informed questions and driving meaningful change. Starr advocates for shifting the review of healthcare expenditures from an annual exercise to a dynamic, quarterly operating conversation. This ongoing dialogue should focus on identifying changes, understanding their root causes, formulating corrective actions, assigning ownership, and establishing metrics for evaluating success.
2. Proactive Management of Variable Cost Drivers
Starr highlights the stark contrast between emergency room (ER) visits and urgent care centers as a prime example of unmanaged variable costs. An average ER visit can cost approximately $2,700, while an urgent care visit for the same clinical need typically costs around $150. Employees often default to ER visits not out of recklessness, but because plan designs fail to differentiate between these settings, and employees lack clear guidance on more cost-effective alternatives.
"Controlling variable costs requires influencing the decision-making process before a claim is even generated," Starr explained. This can be achieved through thoughtful plan design that incentivizes appropriate care settings and through sustained, year-round employee education campaigns, rather than relying solely on a perfunctory annual open enrollment push.
Geographical variations in healthcare delivery also play a significant role. Starr notes that many employers operate under the misconception of having a single, monolithic national employee population. In reality, they often manage numerous distinct local populations, each with its own unique provider markets, access challenges, and social determinants of health. The cost of the same diagnostic category can vary dramatically by state and region, underscoring the need for localized strategies.
3. Directing Employees Toward Higher-Value Care Options
The variability in healthcare provider quality and cost is substantial, yet many health plans treat all providers as interchangeable. This lack of differentiation provides employees with no inherent reason to seek out higher-value options. Starr suggests that strategies such as quality and cost tiering of providers, place-of-service tiering, reference-based pricing, the establishment of centers of excellence for specific conditions, and mandatory pre-procedure second opinions can significantly impact cost and quality. However, the effectiveness of these strategies hinges on employees being aware of and able to access them.
"Would an employee intuitively know the better value choice before a claim occurs?" Starr posed. "If the answer is no, the plan is essentially expecting individuals to make complex healthcare purchasing decisions at a time when they are likely feeling unwell, stressed, or overwhelmed. The objective should be to create a structure where the highest-value clinical option is also the easiest and most intuitive path for your employees."
4. Strategic Management of Metabolic and Chronic Health Conditions as Financial Risks
Starr emphasizes the critical need to view prevalent chronic conditions such as obesity, diabetes, hypertension, and high cholesterol not just as health issues, but as measurable financial risks. Health Action Council’s research indicates that approximately 26 percent of their member employees are diagnosed with obesity, and this demographic accounts for a disproportionately high 46 percent of total healthcare spending. Individuals with obesity incur per-member costs more than double those without the condition. Furthermore, men with a metabolic condition are over seven times more likely to experience a catastrophic health event compared to their counterparts without such conditions.
"If an organization waits until a stroke, a cardiac event, a kidney complication, or a complex diabetes-related admission occurs, an extremely costly claims pathway has already been initiated," Starr warned. "The pertinent question then becomes: what proactive measures are we implementing to reduce the probability, severity, and recurrence of catastrophic claims where early intervention can make a substantial difference?"
5. Governing Pharmacy Expenditures as a Strategic Supply Chain
Starr draws a parallel between pharmacy benefit management and traditional supply chain management, citing the presence of supplier economics, rebates, unit costs, utilization patterns, and critical safety considerations. The administrative fee charged by Pharmacy Benefit Managers (PBMs) represents only the visible tip of the iceberg. The truly impactful financial levers lie in understanding rebate pass-throughs, analyzing spread pricing practices, implementing robust specialty drug management programs, fostering the adoption of biosimil alternatives, enforcing generic-first prescription policies, and addressing the complexities of "polypharmacy." When employees are managing multiple medications prescribed by different physicians for various conditions, the medication list itself can become a significant risk factor, potentially leading to increased side effects, reduced adherence, and a greater likelihood of avoidable ER visits and intensive care unit admissions.
"The fundamental question we must ask is whether we are procuring the lowest net cost medications while ensuring the safest therapeutic regimens," Starr urged. "Pharmacy is a sector too large and too dynamic to be managed solely through procurement activities conducted during contract renewal periods."
Governance: The Force Multiplier for Cost Control
Starr strongly asserts that the success of these five strategic initiatives is contingent upon robust governance structures. Without proper oversight, each individual effort risks becoming an isolated HR project that fails to translate into tangible business outcomes.
In practice, this translates to establishing a quarterly steering committee comprising representatives from finance, HR, procurement, legal, and the organization’s broker or consultant. This committee should operate with a defined agenda focused on population health dashboards, vendor performance scorecards, member experience metrics, and upcoming strategic decisions. For self-insured employers, there is an added legal imperative, as ERISA mandates that fiduciaries act prudently in the best interest of plan participants. This necessitates meticulous documentation of decision-making processes, vendor evaluation methods, and fee monitoring.
Starr concludes that the annual renewal process should serve as a culmination of a year of proactive management, rather than the starting point for strategy development.
The Immediate Agenda: The Next 90 Days
Starr’s most pressing advice to employers is to refrain from waiting for renewal season to begin addressing variable healthcare costs. There are immediate, actionable steps that can be taken to initiate the process of cost containment. These include:
- Data Dive: Immediately request and analyze de-identified claims data from the past 12-24 months. Focus on identifying the top 10-20 diagnoses driving the most cost and the highest claimants.
- Provider Network Review: Assess the current provider network for opportunities to steer employees toward higher-value, lower-cost options. This could involve evaluating tiered networks, centers of excellence, or reference-based pricing strategies.
- Pharmacy Benefit Manager (PBM) Audit: Conduct a thorough review of the PBM contract, focusing on rebate pass-through guarantees, spread pricing transparency, and specialty drug management protocols.
- Chronic Condition Screening and Intervention: Implement or enhance programs that identify and support employees with chronic conditions, such as diabetes prevention or weight management initiatives.
- Employee Education Campaign: Launch a targeted campaign to educate employees about cost-effective care options, the importance of preventive care, and the benefits of utilizing urgent care centers over emergency rooms for non-emergent issues.
Throughout these efforts, maintaining a clear focus on the overarching goal is paramount: "What variable costs are we actively controlling?" This consistent emphasis prevents fragmentation into a multitude of disconnected benefit projects and ensures a direct linkage between implemented actions, actual expenditures, and measurable outcomes.
By adopting all, or even a significant portion, of these strategies, employers can realistically expect to bend the cost curve and achieve substantial savings over the next year.
"Employers are not passive participants in the healthcare system," Starr concluded. "They are active purchasers, fiduciaries with legal obligations, strategic workplace planners, and significant economic actors. Achieving control over healthcare costs is fundamentally about governing a major business expense with unwavering discipline. And, importantly, it is a highly achievable objective."