The landscape of American employer-sponsored healthcare is undergoing its most significant transformation since the inception of the Affordable Care Act (ACA). As of mid-2026, the traditional group health insurance model, which has served as the bedrock of corporate benefits for decades, is increasingly being supplemented or replaced by a more flexible, personalized alternative: the Individual Coverage Health Reimbursement Arrangement (ICHRA). This shift represents a fundamental change in how businesses manage medical costs and how employees access care, signaling a move toward a consumer-driven healthcare economy.
Data from the first half of 2026 indicates that the adoption of ICHRAs has accelerated at an unprecedented rate. Between 2024 and 2025, adoption among small employers surged by 52%, while mid-sized and large enterprises saw increases ranging from 34% to 49%. Federal government estimates now project that by 2032, millions of American workers will have transitioned from traditional group plans to individual market coverage supported by employer-funded HRA accounts. This transition is not merely a budgetary adjustment; it is a structural realignment of the healthcare industry.
The Economic Drivers of the ICHRA Surge
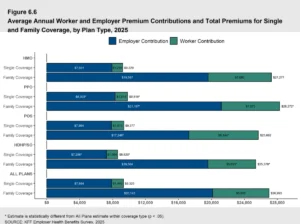
The primary catalyst for this migration is the unsustainable trajectory of group health insurance premiums. In 2025, the average annual premium for employer-sponsored group coverage reached $9,325 for self-only enrollment and a staggering $26,993 for family coverage. These figures represent year-over-year increases of 5% and 6%, respectively. When contrasted against a 4% rise in average employee wages and a 2.7% inflation rate, the disparity highlights a growing financial burden on both corporations and their staff.
For small businesses, the stakes are even higher. Recent surveys suggest that nearly 47% of small firms currently offering group coverage would be forced to terminate their benefits if premiums were to increase by an additional 15%. This "breaking point" has led many organizations to seek the ICHRA as a lifeline. Unlike group plans, where employers are at the mercy of annual rate hikes determined by carriers, the ICHRA allows employers to set a fixed monthly contribution. This "defined contribution" model provides budgetary predictability, capping the employer’s financial risk while still providing tax-free funds to employees for medical expenses.
A Chronology of Regulatory Evolution
The rise of the ICHRA was not an overnight phenomenon but the result of a multi-year regulatory evolution aimed at expanding health benefit options.
- 2010: The passage of the Affordable Care Act established the individual marketplace, creating a foundation for portable health insurance.
- 2016: The 21st Century Cures Act introduced the Qualified Small Employer Health Reimbursement Arrangement (QSEHRA), allowing small businesses to reimburse for individual premiums, though with strict contribution limits.
- 2019: Federal agencies (Treasury, Labor, and Health and Human Services) issued a final rule creating the ICHRA. This new HRA removed the size restrictions of the QSEHRA and allowed for higher contribution limits, provided employees purchased ACA-compliant individual coverage.
- 2020: The ICHRA became available for use on January 1, 2020, though initial adoption was slowed by the global pandemic.
- 2021–2024: As remote work became standardized and the "Gig Economy" expanded, the need for portable, individual-centric benefits grew.
- 2025–2026: Widespread adoption across all business sizes occurred as insurance carriers expanded their individual market offerings to meet the demand from ICHRA-funded consumers.
Mechanisms of the ICHRA Model
To understand the impact on the industry, one must understand how the ICHRA functions as a financial vehicle. An ICHRA is an IRS-compliant health benefit that allows businesses of any size to reimburse employees tax-free for their individual health insurance premiums and qualified out-of-pocket medical expenses.
The process typically follows a three-step cycle. First, the employer establishes a monthly allowance for each employee, which can be tiered based on legitimate job-based categories (such as full-time vs. part-time or geographic location). Second, the employee selects and pays for their own individual health insurance plan on the open market or a state exchange. Third, the employee submits proof of their premium or medical expense, and the employer provides a tax-free reimbursement up to the allowed amount.
Crucially, the ICHRA requires employees to maintain enrollment in individual health insurance to remain eligible. This ensures that the risk pool remains stable and that employees are not left uninsured. For retirees, IRS Notice 2002-45 allows for similar HRA structures, providing a bridge for those transitioning out of the active workforce.
Market Disruption: Competition and Individual Choice
One of the most profound impacts of the ICHRA is the revitalization of the individual insurance market. Historically, insurance carriers focused their most competitive pricing and robust provider networks on the "Large Group" market, where they could secure thousands of lives in a single contract. This left the individual market as a secondary priority.
However, the influx of ICHRA participants is shifting the power dynamic. Carriers must now compete for the business of the individual consumer rather than the HR director of a corporation. This competition has led to a diversification of plan options. In 2025, while 66% of employers offering group plans provided only one choice to their staff, 97% of individuals shopping on the individual market had access to three or more qualified health plan issuers.

Data from the 2026 National ICHRA Report reveals that employees using an ICHRA chose an average of 14 different plans per employer. This indicates that when given the choice, employees do not opt for a "one-size-fits-all" solution. Instead, they select plans that align with their specific preferred physicians, prescription needs, and financial thresholds.
Portability and the Future of the American Workforce
The ICHRA addresses a long-standing criticism of the American healthcare system: the "job lock" created by employer-linked insurance. In the traditional model, if an employee leaves their job, they lose their health plan, their progress toward their deductible resets, and they may lose access to their doctors.
In the modern labor market, where the Bureau of Labor Statistics (BLS) reports that the average worker changes jobs every 3.9 years, the ICHRA offers a solution through portability. Because the individual owns the insurance policy, the plan stays with them regardless of their employment status. While the employer’s reimbursement stops when the employee leaves, the coverage remains active as long as the individual continues to pay the premiums. This continuity of care reduces disruptions in chronic disease management and prevents the administrative burden of switching plans mid-year.
Public Health and Community Impact
The expansion of ICHRAs is also contributing to the stabilization of health outcomes in local communities. Historically, younger and healthier individuals—often referred to as "invincibles"—frequently opted out of expensive group plans. The ICHRA, however, has proven popular among younger demographics.
According to the HRA Council, the age distribution of HRA enrollees in 2024 showed significant engagement from younger workers:
- Under 25: 11%
- 25–34: 21%
- 35–44: 21%
- 45–54: 19%
- 55–64: 24%
- 65+: 4%
By bringing younger, lower-risk individuals into the individual market, the ICHRA helps balance the risk pool, which exerts downward pressure on premiums for everyone, including those with pre-existing conditions. Furthermore, by making coverage more affordable, the ICHRA has helped reduce the percentage of adults who skip medical care due to cost—a figure that stood at 26% in 2025.
Geographic hotspots for ICHRA adoption, such as New York City, Atlanta, and Los Angeles, are seeing a correlated increase in the utilization of preventive services. As more individuals gain access to routine screenings and early interventions, the broader healthcare system experiences a reduction in the burden of untreated chronic illnesses and preventable emergency room visits.
Expert Analysis and Future Outlook
Industry analysts suggest that the "ICHRA Revolution" is only in its middle chapters. The shift represents a move toward "healthcare consumerism," where the end-user is more engaged in the cost and quality of their care. This engagement is expected to drive further transparency in medical pricing, as consumers armed with their own health plans shop for value in imaging, labs, and elective procedures.
However, the transition is not without challenges. For the ICHRA model to reach its full potential, the individual market must remain robust and competitive. While the expiration of certain federal premium tax credits in early 2026 led to a slight dip in overall ACA market enrollments, the steady influx of ICHRA-funded participants has provided a necessary floor for market stability.
For employers, the transition requires a change in mindset from "providing a plan" to "providing a budget." Companies like PeopleKeep and Remodel Health have emerged as critical infrastructure in this new era, providing the software necessary to manage the complex compliance and reimbursement requirements of the IRS.
As the U.S. moves toward 2032, the ICHRA is poised to become the standard for health benefits in the same way the 401(k) replaced the traditional pension. By decoupling the choice of insurance from the source of employment, the ICHRA is creating a more resilient, portable, and personalized healthcare ecosystem for the American worker. The result is a system that is not only more sustainable for the employer’s bottom line but more responsive to the diverse medical and financial needs of the modern workforce.