For decades, the bedrock of the American healthcare system has been the employer-sponsored group health insurance plan. According to data from KFF, approximately 60% of the United States population—representing roughly 165.6 million individuals—relied on their employers for medical coverage in 2025. This long-standing tradition of linking employment to healthcare access has shaped the economic landscape of the country, yet as medical costs continue to climb, the traditional model is facing unprecedented scrutiny. While the majority of the workforce is familiar with the concept of a "group plan," the underlying mechanics, historical drivers, and emerging alternatives are often less understood by the business owners tasked with funding them.
The Mechanics of Group Health Insurance
A group health insurance plan is a centralized policy purchased by an employer or organization and offered to its members, typically employees and their dependents. Unlike individual insurance, which a person buys directly from a carrier or a public exchange, group coverage is built on the principle of risk pooling. By grouping a large number of individuals together, the insurance provider can spread the financial risk across the entire population. This theoretically allows for lower premiums, as the high costs associated with a few high-need members are balanced by the lower costs of healthier members.
Employers generally procure these plans through insurance brokers or directly from carriers. In some instances, particularly among larger corporations, the organization may choose to "self-fund" the benefit. In a self-funded model, the employer pays for medical claims out-of-pocket rather than paying fixed premiums to an insurer, often hiring a third-party administrator (TPA) to manage the logistics. To mitigate the risk of catastrophic claims, self-funded employers typically purchase stop-loss insurance, which kicks in once claims exceed a certain threshold.
The variety of plans available to employers has expanded over the years to include several distinct network structures:
- Health Maintenance Organizations (HMOs): These require members to use a specific network of doctors and hospitals and usually necessitate a referral from a primary care physician to see a specialist.
- Preferred Provider Organizations (PPOs): These offer more flexibility, allowing members to see out-of-network providers at a higher cost without needing a referral.
- Exclusive Provider Organizations (EPOs): A hybrid model that generally does not cover out-of-network care except in emergencies but does not require referrals for specialists.
- Point of Service (POS) Plans: These require members to choose a primary care physician but allow for out-of-network care with a referral, albeit at a higher cost.
To control rising costs, many organizations have shifted toward High-Deductible Health Plans (HDHPs). While these plans offer lower monthly premiums, they require employees to pay significantly more out-of-pocket before insurance coverage begins.
A Chronological History of Employer-Sponsored Care
The evolution of the American health insurance system is a result of historical accidents and legislative interventions rather than a singular master plan. The timeline of this development reveals how the U.S. became an outlier in its reliance on employer-based coverage.
1798: The U.S. Marine Hospital Service is established, marking the first recorded instance of a government-mandated health plan for a specific group of workers (seamen).
Early 20th Century: Most Americans paid for medical care out-of-pocket. Hospitals began offering "pre-paid" plans to local groups, such as teachers or miners, to ensure a steady stream of revenue during the Great Depression.
1942-1945: During World War II, the federal government implemented the Emergency Price Control Act to prevent inflation. This included strict wage freezes. To attract workers during a labor shortage without violating wage caps, employers began offering fringe benefits, including health insurance. The War Labor Board ruled that these benefits did not count as wages.
1954: The Internal Revenue Service (IRS) codified the tax-exempt status of employer-sponsored health insurance. This meant that employer contributions toward premiums were tax-deductible for the business and not counted as taxable income for the employee. This solidified the group plan as the dominant model for American healthcare.
1974: The Employee Retirement Income Security Act (ERISA) was passed, providing federal standards for private pension and health plans. This allowed large employers to self-insure while being exempt from many state-level insurance mandates.
2010: The Affordable Care Act (ACA) introduced the "Employer Mandate," requiring businesses with 50 or more full-time equivalent (FTE) employees to provide "minimum essential coverage" that is "affordable" or face financial penalties.
The Economic Burden of Rising Premiums
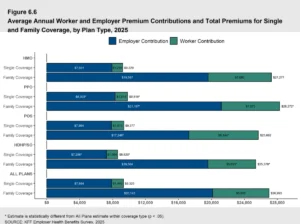
The sustainability of the traditional group model is currently being tested by the relentless rise in healthcare costs. Data from 2025 indicates that the average annual premium for employer-sponsored insurance reached $9,325 for single coverage and $26,993 for family coverage. These costs are typically shared between the employer and the employee, but the increasing weight of these premiums is squeezing both parties.

For small and mid-sized enterprises (SMEs), these costs can be prohibitive. Unlike large corporations with thousands of employees, small businesses lack the bargaining power to negotiate favorable rates with insurance carriers. Furthermore, a single catastrophic illness within a small group can lead to double-digit premium increases during the next renewal cycle. This volatility makes long-term budgeting difficult for small business owners and can lead to a "death spiral" where rising costs force healthier employees to opt-out, further driving up premiums for those who remain.
Regulatory Requirements and the ACA Mandate
While many employers offer health insurance as a recruitment tool, for large organizations, it is a legal requirement. Under the ACA, Applicable Large Employers (ALEs)—defined as those with 50 or more FTEs—must offer coverage to at least 95% of their full-time workforce.
To satisfy the mandate, the coverage must meet two primary criteria:
- Minimum Value: The plan must pay for at least 60% of the total allowed cost of covered services.
- Affordability: The employee’s share of the premium for the lowest-cost self-only plan cannot exceed a certain percentage of their household income (a threshold adjusted annually by the IRS).
Failure to comply with these regulations can result in Employer Shared Responsibility Provisions (ESRP) penalties, which can amount to millions of dollars for the largest firms.
The Shift Toward Personalized Alternatives
In response to the limitations of the "one-size-fits-all" group model, a new wave of personalized health benefits has emerged. These alternatives aim to provide employees with more choice while giving employers more control over their budgets.
Individual Coverage Health Reimbursement Arrangements (ICHRA)
Introduced via federal rule changes in 2020, the ICHRA allows employers of any size to reimburse employees tax-free for individual health insurance premiums and other medical expenses. Instead of choosing a single plan for the entire company, the employer sets a monthly allowance. Employees then shop for a plan on the individual market that fits their specific needs—choosing their own doctors, networks, and deductible levels.
Qualified Small Employer Health Reimbursement Arrangements (QSEHRA)
Designed specifically for businesses with fewer than 50 employees that do not offer a group plan, the QSEHRA functions similarly to an ICHRA but has annual contribution limits set by the IRS. It provides a way for small businesses to help employees with medical costs without the administrative burden of managing a full insurance policy.
Health Stipends
Some organizations choose to offer a flat health stipend. While highly flexible and easy to administer, stipends are considered taxable income. Furthermore, they do not satisfy the ACA employer mandate for larger firms, making them more common among startups and very small businesses.
The Impact of a Multi-State and Remote Workforce
The rise of remote work has further complicated the administration of traditional group plans. When an organization has employees scattered across multiple states, finding a single insurance carrier with an adequate provider network in every location becomes a logistical nightmare. Traditional HMOs and PPOs are often tied to specific geographic regions.
Employers with distributed teams are increasingly turning to HRAs because they solve the "network" problem. Since employees purchase individual plans in their own local markets, the employer no longer needs to worry about whether a doctor in Oregon is in-network for a company based in New York.
Fact-Based Analysis of Broader Implications
The transition away from traditional group health insurance toward reimbursement models like the ICHRA represents a fundamental shift in the employer-employee relationship. This "defined contribution" model—similar to the shift from traditional pensions to 401(k) plans—transfers the responsibility of plan selection to the individual while allowing the employer to cap their financial exposure.
From a market perspective, this shift could strengthen the individual insurance exchanges by bringing in a younger, healthier pool of participants who were previously covered under group plans. For employees, the primary benefit is portability; an individual plan belongs to the worker, not the company, meaning coverage doesn’t necessarily end the moment they leave a job.
However, the transition is not without challenges. It requires a higher level of "health literacy" from employees, who must now navigate the complexities of the insurance marketplace themselves. This has led to the growth of specialized administration platforms designed to automate the compliance and reimbursement process for businesses, ensuring that HRAs are managed according to IRS and Department of Labor guidelines.
Conclusion
The landscape of American employee benefits is in the midst of a significant transformation. While group health insurance remains the dominant form of coverage, the economic pressures of rising premiums and the logistical demands of a remote workforce are driving a move toward more flexible, individualized solutions. For employers, the choice between a traditional group plan and a modern alternative like an HRA is no longer just a financial decision; it is a strategic one that impacts their ability to attract talent, maintain compliance, and ensure the long-term viability of their organization. As we move further into the decade, the "one-size-fits-all" approach to healthcare appears increasingly likely to be replaced by a model that prioritizes personalization and cost predictability.