As global healthcare expenditures continue their decades-long upward trajectory, enterprises of all sizes are confronting a critical inflection point in benefits administration. The traditional model of one-size-fits-all group health insurance is increasingly viewed as an unsustainable financial burden for many small to mid-sized organizations. In response to these fiscal pressures, Health Reimbursement Arrangements (HRAs) have emerged as a cornerstone of the modern "defined contribution" approach to employee wellness. By shifting from a fixed-benefit model to a fixed-contribution model, employers are gaining unprecedented control over their budgets while simultaneously providing employees with the flexibility to personalize their healthcare coverage.
The Economic Landscape of Modern Healthcare Benefits
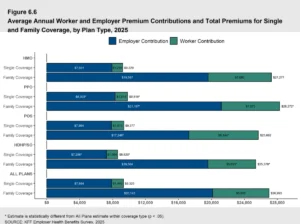
The shift toward HRAs is driven primarily by the escalating cost of traditional group premiums. According to historical data from the Kaiser Family Foundation and more recent market projections for 2026, the average annual premium for family coverage has consistently outpaced inflation, often rising by 4% to 7% annually. For many small business owners, these increases necessitate either a reduction in coverage quality or an increase in the employee’s share of the premium—both of which can negatively impact talent retention and morale.
An HRA serves as a tax-advantaged vehicle that allows employers to set aside a specific monthly allowance for employees’ out-of-pocket medical expenses. Unlike traditional insurance, where the employer pays a premium to an insurance company regardless of how much care is consumed, an HRA only requires the employer to pay when an employee actually incurs a qualified medical expense. This "pay-as-you-go" structure, combined with significant tax advantages—reimbursements are generally tax-free for employees and tax-deductible for employers—has positioned the HRA as a primary alternative to conventional health plans.
A Chronological Evolution of Reimbursement Models
The regulatory framework governing HRAs has evolved significantly over the last two decades, reflecting a bipartisan effort to modernize the American healthcare system.
- 2002: The Foundation: The Internal Revenue Service (IRS) issued formal guidance (Notice 2002-45) that solidified the tax-exempt status of HRAs, provided they were funded solely by the employer and used for substantiated medical expenses.
- 2010: The Affordable Care Act (ACA) Impact: The ACA initially placed restrictions on certain types of HRAs, particularly stand-alone arrangements, as they were often viewed as failing to meet "minimum essential coverage" (MEC) requirements on their own.
- 2016: The 21st Century Cures Act: Recognizing the plight of small businesses, Congress passed this act to create the Qualified Small Employer HRA (QSEHRA). This allowed companies with fewer than 50 employees to offer a stand-alone benefit for the first time since the ACA’s implementation.
- 2020: The ICHRA Expansion: Federal departments finalized rules for the Individual Coverage HRA (ICHRA), a highly flexible tool available to employers of all sizes. This marked a major shift toward the "defined contribution" model, allowing employers to move away from group plans entirely.
- 2024–2026: Technological Integration: The current era is defined by the rise of specialized administration platforms that automate compliance and reimbursement, making these complex tax vehicles accessible to non-specialist HR departments.
The Mechanics of Integrated HRAs: GCHRA and EBHRA
Integrated HRAs are designed to function in tandem with an existing group health insurance policy. They are primarily utilized to mitigate the impact of high-deductible health plans (HDHPs) on the workforce.
The Group Coverage HRA (GCHRA)
The GCHRA is the most common form of integrated HRA. It allows an employer to maintain a traditional group plan while setting aside additional funds to cover the "gap" created by high deductibles or co-insurance. For example, an employer might switch to a lower-premium HDHP to save on monthly costs and then use a GCHRA to reimburse employees for the first $2,000 of their deductible.
A critical advantage of the GCHRA is its customizability. Employers can divide their workforce into "employee classes"—such as salaried versus hourly or geographic locations—and offer different reimbursement levels to each. However, GCHRAs cannot be used to reimburse health insurance premiums; they are strictly for out-of-pocket medical expenses.
The Excepted Benefit HRA (EBHRA)
The EBHRA is a more specialized tool. It allows employers to provide up to a federally capped annual amount to reimburse employees for "excepted benefits" that are not usually covered by a primary health plan. This includes dental and vision care, long-term care, or premiums for COBRA and short-term disability insurance. Notably, an employee does not have to be enrolled in the primary group plan to utilize an EBHRA, though the employer must offer a group plan to the workforce.
The Rise of Stand-Alone Alternatives: ICHRA and QSEHRA
For organizations looking to exit the business of managing group plans entirely, stand-alone HRAs offer a path to total premium control.
The Individual Coverage HRA (ICHRA)
The ICHRA is widely considered the most disruptive force in employee benefits today. It allows employers of any size to give employees a tax-free allowance to buy their own health insurance on the individual market.

Industry analysts point to the "portability" of the ICHRA as its greatest strength. If an employee leaves the company, they take their individual insurance policy with them, ensuring continuity of care. For the employer, the ICHRA eliminates the "renewal shock" associated with annual group plan negotiations. Because there are no maximum contribution limits, the ICHRA is as scalable as a traditional 401(k) plan.
The Qualified Small Employer HRA (QSEHRA)
Specifically tailored for small businesses with fewer than 50 full-time equivalent employees, the QSEHRA is a "turnkey" solution for startups and small firms. Unlike the ICHRA, the QSEHRA has annual contribution limits set by the IRS. It requires that the employer offer the benefit on the same terms to all eligible employees, ensuring a high level of fairness. If an employee does not use their full allowance by the end of the year, the funds remain with the employer, further protecting the company’s bottom line.
Statistical Overview: The Impact of Transitioning to HRAs
Data from 2025 benefit surveys indicates that small to mid-sized businesses (SMBs) transitioning from group plans to ICHRAs or QSEHRAs saw an average reduction in administrative overhead of approximately 15% to 20%. Furthermore, by moving to a defined contribution model, employers were able to accurately forecast their healthcare spending for the next 36 months with a 98% accuracy rate, compared to the volatility of group plan renewals which can fluctuate by double digits unexpectedly.
From the employee perspective, the results are more nuanced. While some employees prefer the "pre-packaged" nature of group plans, a growing segment of the workforce—particularly Millennial and Gen Z employees—values the ability to choose a plan that includes their specific preferred doctors and specialists. In markets with robust individual exchanges, employees using an ICHRA often find they have access to a wider variety of plans than their employer could have offered through a single group policy.
Compliance, Regulatory Oversight, and Administration
Despite their benefits, HRAs are subject to a complex web of federal regulations, including ERISA (Employee Retirement Income Security Act), HIPAA (Health Insurance Portability and Accountability Act), and various IRS codes.
"The primary risk for employers is not the cost of the benefit, but the cost of non-compliance," states a recent industry analysis on benefits administration. Employers who attempt to self-administer an HRA often run afoul of HIPAA privacy rules, which prohibit employers from seeing an employee’s private medical receipts. To mitigate this risk, most organizations now utilize third-party administration (TPA) software. These platforms act as a firewall, verifying that an expense is legitimate and reimbursable under IRS rules without revealing sensitive medical data to the employer.
Key compliance areas include:
- Legal Documentation: Each HRA must have a formal plan document and a Summary Plan Description (SPD).
- Nondiscrimination Testing: Employers must ensure that the HRA does not unfairly favor highly compensated employees.
- MEC Verification: For stand-alone HRAs, administrators must verify that employees have "minimum essential coverage" before issuing reimbursements.
Broader Impact and Implications for the Future of Work
The rise of HRAs reflects a broader trend toward the personalization of the employment contract. In a remote-first and globalized economy, the traditional group plan—often tied to a specific geographic network—is becoming obsolete. HRAs allow a company headquartered in New York to provide the same level of healthcare support to a remote employee in Texas or a digital nomad in Florida by letting them purchase local coverage.
As we move toward the late 2020s, the "consumerization" of healthcare is expected to accelerate. Analysts predict that by 2030, defined contribution healthcare will be as standard as the 401(k) is for retirement. This shift places more responsibility on the employee to navigate the healthcare market, but it also provides them with the financial tools to do so effectively.
In conclusion, the choice between integrated and stand-alone HRAs is not merely a financial decision but a strategic one. Organizations that prioritize flexibility, budget stability, and employee choice are increasingly finding that the HRA model provides a sustainable path forward in an era of unpredictable healthcare costs. Whether used to bolster an existing plan or as a complete replacement for traditional insurance, these arrangements represent the next chapter in the evolution of corporate wellness and fiscal responsibility.