The landscape of American workforce compensation is undergoing a fundamental transformation as small and mid-sized enterprises (SMEs) grapple with the escalating costs of traditional healthcare. For decades, the "one-size-fits-all" group health insurance model served as the gold standard for corporate benefits. However, as of early 2026, a significant pivot toward "defined contribution" models—specifically Health Reimbursement Arrangements (HRAs)—is reshaping how employers attract and retain talent in an increasingly competitive labor market.
The traditional group health insurance model has long been criticized for its lack of flexibility and its prohibitive cost structure. Many small businesses find themselves priced out of the market or forced to offer plans with high deductibles that leave employees functionally uninsured for minor medical needs. In response, the adoption of stand-alone HRAs has surged, offering a mechanism through which employers can provide tax-free medical stipends, allowing employees to purchase individual plans that cater to their specific household requirements.
The Evolution of the HRA: A Regulatory Chronology
The transition toward HRAs did not happen in a vacuum. It is the result of over two decades of regulatory evolution aimed at decoupling health insurance from specific employers.
The journey began in 2002 with IRS Revenue Ruling 2002-45, which officially recognized HRAs as employer-funded arrangements to reimburse medical expenses. However, the implementation of the Affordable Care Act (ACA) in 2010 initially restricted the use of stand-alone HRAs, as they were often seen as failing to meet "market reform" requirements.
The tide turned significantly in December 2016 with the passage of the 21st Century Cures Act, which established the Qualified Small Employer Health Reimbursement Arrangement (QSEHRA). This allowed businesses with fewer than 50 full-time employees to offer tax-free reimbursements for premiums and medical costs without the penalties previously associated with stand-alone plans.
By 2019, further deregulation led to the creation of the Individual Coverage Health Reimbursement Arrangement (ICHRA). Effective January 1, 2020, the ICHRA expanded the HRA concept to businesses of all sizes, allowing them to replace traditional group plans entirely with a flexible, allowance-based system. This chronology highlights a clear legislative trend toward personalized, portable benefits that prioritize employee choice over corporate procurement.
Understanding the Mechanics of Stand-Alone HRAs
At its core, a stand-alone HRA is an employer-funded, tax-advantaged health benefit. Unlike a traditional plan, where the employer selects a carrier and a specific set of benefits for the entire staff, the HRA allows the employer to set a fixed monthly allowance. Employees then use these funds to purchase their own individual health insurance on the open market or via a state exchange.
There are two primary vehicles for this strategy:
- The Qualified Small Employer HRA (QSEHRA): Specifically designed for companies with fewer than 50 full-time equivalent employees. It requires that the employer does not offer a group plan and that the benefit be offered on the same terms to all eligible employees, though allowances may vary based on age or family size.
- The Individual Coverage HRA (ICHRA): Available to companies of any size. It offers greater flexibility, allowing employers to create "classes" of employees (such as full-time, part-time, or seasonal) and offer different allowance amounts to each class.
In both scenarios, the contributions are tax-deductible for the employer and 100% tax-free for the employee, provided they maintain minimum essential coverage (MEC). This "defined contribution" approach provides budget predictability for the business while empowering the employee to act as a consumer of their own healthcare.
Comparative Analysis: Traditional Insurance vs. HRA Coverage
To understand the value proposition of an HRA, one must examine what traditional insurance typically covers versus the expanded scope of an HRA.
Traditional group health insurance plans are designed primarily to cover "essential health benefits" as defined by the ACA. These include preventive care, emergency services, hospitalization, and maternity care. However, the level of coverage is dictated by the plan’s "metallic tier." A Bronze plan, for instance, typically has an actuarial value of 60%, leaving the employee to cover 40% of their costs through deductibles and coinsurance. A Gold plan raises that value to 80%, but at a significantly higher premium cost to the employer.
The HRA serves as a financial bridge. While the individual insurance plan purchased by the employee covers the major medical events, the HRA allowance can be used to reimburse the out-of-pocket costs that the insurance plan ignores.

Typical Insurance Coverage Includes:
- Preventive Care: Routine check-ups, immunizations, and screenings.
- Outpatient Care: Visits to primary care physicians and specialists.
- Emergency Services: Ambulance rides and ER visits.
- Prescription Drugs: Though often subject to complex formularies and tiered pricing.
- Mental Health: Counseling and substance use disorder services.
Expanded HRA Reimbursement Capabilities:
The HRA goes beyond the "major medical" scope. Under IRS Publication 502 and the enhancements provided by the CARES Act, HRAs can reimburse:
- Individual Insurance Premiums: Often the most significant expense for an employee.
- Dental and Vision: Including braces, LASIK, and routine cleanings which are frequently excluded from standard medical plans.
- Over-the-Counter (OTC) Items: Since the 2020 CARES Act, items like pain relievers, cold medicine, and menstrual care products are eligible without a prescription.
- Medical Equipment: Crutches, blood pressure monitors, and even hearing aid batteries.
- Holistic Treatments: Acupuncture and chiropractic care, provided they are deemed medically necessary.
Supporting Data: The Economic Case for HRAs
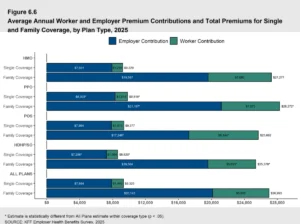
Recent data from the Kaiser Family Foundation (KFF) indicates that the average annual premium for employer-sponsored family health coverage reached nearly $25,000 in 2025, a trend that has continued into 2026. For many small businesses, these costs are unsustainable.
Industry analysis suggests that employers switching from traditional group plans to an ICHRA model can save an average of 15% to 20% on annual benefit expenditures. This saving is primarily driven by the elimination of "utilization risk." In a group plan, one or two high-cost claims from employees can cause the entire group’s premiums to skyrocket the following year. In an HRA model, the employer’s liability is capped at the allowance amount, regardless of the employees’ actual medical claims.
Furthermore, a 2025 survey of employees using HRAs found that 72% preferred the ability to choose their own plan over a standard company-offered plan. This shift in sentiment is largely attributed to the rise of the "gig economy" and remote work, where employees may live in different regions with different provider networks.
Compliance and Non-Eligible Expenses
While HRAs offer immense flexibility, they are governed by strict IRS guidelines. To maintain the tax-advantaged status, reimbursements must be for "medically necessary" expenses. The IRS explicitly excludes "general health" or cosmetic expenses from HRA eligibility.
Common Non-Eligible Expenses Include:
- Cosmetic Procedures: Facelifts, hair transplants, or teeth whitening.
- General Wellness: Gym memberships, health club dues, or weight loss programs (unless prescribed to treat a specific disease like hypertension).
- Insurance Premiums for Non-Qualified Plans: Such as life insurance or "accident-only" policies.
- Non-Medical Travel: Transportation to a pharmacy or general travel for "relaxation" purposes.
Employers must ensure they have a robust verification process in place—often managed by third-party administrators—to review receipts and invoices before funds are disbursed. Failure to comply with these standards can result in the entire HRA being deemed a taxable benefit, leading to significant payroll tax liabilities.
Broader Implications for the Future of Work
The rise of stand-alone HRAs represents a broader socio-economic shift toward the "portability" of benefits. In a labor market characterized by frequent job-hopping and a desire for autonomy, the HRA model allows an employee’s healthcare to remain constant even if their employer changes, provided they keep their individual plan.
For employers, the HRA is more than just a cost-saving measure; it is a strategic tool for talent acquisition. By offering a benefit that covers "everyday" health needs—like contact lenses or over-the-counter allergy medication—companies can demonstrate a more holistic commitment to employee well-being than a traditional plan that only "kicks in" during a catastrophic event.
As we move toward 2027, analysts predict that the ICHRA market will continue to expand, particularly in industries with high proportions of part-time or hourly workers who have historically been excluded from traditional benefits. The "democratization" of health benefits through HRAs is likely to remain a defining feature of the American corporate landscape for the foreseeable future.
In conclusion, while traditional group health insurance will likely remain a fixture for large corporations with massive risk pools, the stand-alone HRA has emerged as the superior choice for the modern, agile business. By prioritizing flexibility, tax efficiency, and employee choice, HRAs provide a sustainable path forward in an era of unpredictable healthcare costs. Organizations looking to modernize their benefits package should view the HRA not merely as an alternative, but as a primary strategy for long-term fiscal health and employee satisfaction.