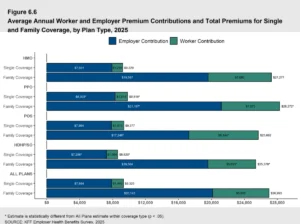
The landscape of American corporate benefits is undergoing a seismic shift as rising health insurance premiums continue to outpace inflation and wage growth. According to data from the Kaiser Family Foundation’s 2023 Employer Health Benefits Survey, the average premium for family coverage has risen 22% over the last five years, reaching nearly $24,000 annually. In response to these escalating costs, an increasing number of organizations are abandoning the traditional "one-size-fits-all" group health insurance model in favor of "defined contribution" strategies. These strategies, primarily executed through Health Reimbursement Arrangements (HRAs) and health stipends, allow employers to control their budgetary exposure while offering employees the autonomy to select insurance products that align with their specific medical needs and geographic locations. However, the choice between these two models involves complex considerations regarding Internal Revenue Service (IRS) compliance, tax liabilities, and federal mandates under the Affordable Care Act (ACA).
The Fundamental Distinction: HRAs versus Health Stipends
At the core of the debate between HRAs and health stipends is the distinction between a formal health plan and a cash-based benefit. A Health Reimbursement Arrangement is an employer-funded, tax-advantaged health benefit plan that reimburses employees for out-of-pocket medical expenses and, in some cases, individual insurance premiums. Because the IRS classifies a properly structured HRA as a "group health plan," the reimbursements are generally excluded from the employee’s gross income and are tax-deductible for the employer.
In contrast, a health stipend is essentially a recurring financial allowance provided to employees to assist with medical costs. Unlike the HRA, a stipend is not a formal health insurance plan. The IRS views these funds as additional taxable wages. While stipends offer maximum flexibility and minimal administrative burden, they do not provide the tax efficiencies that have made HRAs a cornerstone of modern benefits administration.
Tax Implications and the Mechanism of Reimbursement
The financial implications of choosing one model over the other are significant for both the corporate bottom line and the employee’s take-home pay. For an HRA to maintain its tax-exempt status, it must adhere strictly to IRS regulations and the Employee Retirement Income Security Act (ERISA). When these conditions are met, the employer avoids paying the 7.65% Federal Insurance Contributions Act (FICA) tax on the reimbursed amounts, and the employee receives the funds without being subject to federal income tax or payroll taxes.
For example, if an employer intends to provide an employee with a $500 monthly benefit for healthcare, the HRA model requires a straight $500 outlay. However, because a health stipend is treated as taxable income, the employer must "gross up" the payment if they want the employee to receive a net value of $500. After accounting for the employer’s share of FICA and the employee’s income and payroll tax obligations, a $500 net stipend could cost the employer between $650 and $680. This 30% to 36% "tax drag" makes stipends a significantly more expensive way to deliver the same level of support.
A Chronology of Regulatory Evolution
The current framework for these benefits is the result of over a decade of legislative and regulatory changes. Understanding this timeline is essential for compliance:
- 2010: The Affordable Care Act (ACA) Passed: The ACA introduced market reforms that initially made it difficult for employers to reimburse individual premiums, as these arrangements were often seen as failing to meet the law’s "no annual limit" and "preventive care" requirements.
- 2013-2015: IRS Guidance on Employer Payment Plans: The IRS issued several notices (including Notice 2013-54) stating that "employer payment plans" that reimbursed individual market premiums generally failed to comply with ACA reforms, leading to potential excise taxes of $100 per day per employee.
- 2016: The 21st Century Cures Act: Recognizing the burden on small businesses, Congress passed this bipartisan legislation to create the Qualified Small Employer Health Reimbursement Arrangement (QSEHRA). This allowed businesses with fewer than 50 full-time equivalent (FTE) employees to reimburse individual premiums tax-free.
- 2019-2020: The Expansion of HRAs: Federal agencies issued new rules creating the Individual Coverage HRA (ICHRA). This expanded the HRA concept to businesses of all sizes, allowing them to offer an HRA in lieu of traditional group insurance, provided employees purchase qualifying individual coverage.
- 2020: The CARES Act: This legislation expanded the definition of "qualified medical expenses" under IRS Publication 502 to include over-the-counter medications and menstrual care products without a prescription, further increasing the utility of HRAs.
Compliance Requirements for HRAs
For an organization to successfully implement an HRA, it must satisfy specific criteria regarding coverage and documentation. For a QSEHRA, employees must maintain Minimum Essential Coverage (MEC) to receive tax-free reimbursements. If an employer mistakenly reimburses an employee who lacks MEC, that reimbursement becomes taxable income for the employee.
The ICHRA carries even stricter requirements. To be eligible for an ICHRA, an employee must be enrolled in individual health insurance that meets MEC standards. This excludes "short-term, limited-duration insurance" (STLDI) and healthcare sharing ministries. Furthermore, employers must provide a written notice to eligible employees at least 90 days before the beginning of the plan year, explaining the terms of the ICHRA and how it might affect their eligibility for the Premium Tax Credit (PTC) on the federal or state marketplace.
The Role of Health Stipends in the Modern Workplace
Despite the tax disadvantages, health stipends remain a viable tool for specific organizational needs. Small startups or businesses with a high percentage of part-time or seasonal workers often utilize stipends because they require no formal plan documents and no reporting under the ACA’s employer mandate.
Because the ACA prohibits "Employer Payment Plans" that are not formal HRAs, an employer cannot legally require an employee to use a stipend to purchase health insurance. If an employer demands proof of a health insurance receipt as a condition for receiving a stipend, they risk violating ACA market reforms. Consequently, stipends are typically offered as "unrestricted" funds, even if the employer’s intent is for the money to be used for wellness or medical costs.
Stipends are also an effective "bridge" for employees who are already receiving significant Premium Tax Credits. Since receiving funds through an ICHRA can disqualify an individual from receiving marketplace subsidies, some employees may prefer a taxable stipend that supplements their out-of-pocket costs without triggering a loss of their federal subsidy.
Broader Impact and Strategic Implications
The shift toward HRAs and stipends reflects a broader trend toward the "personalization of benefits." In a competitive labor market, the ability for an employee in New York to choose a different plan than an employee in Texas—while the employer maintains a consistent budget—is a powerful recruitment tool.
Industry analysts suggest that the ICHRA, in particular, is poised to disrupt the traditional group market. By shifting the risk to the individual insurance market, employers are protected from "claims shock"—the sudden premium spikes that occur when a single employee incurs catastrophic medical bills. For the employee, the HRA model provides "portability." If they leave the company, they can often keep their individual insurance policy, simply taking over the premium payments themselves, rather than dealing with the complexities and high costs of COBRA.
However, the administrative complexity of managing reimbursements, verifying receipts, and ensuring compliance with IRS Publication 502 means that many employers utilize third-party administrators (TPAs). These platforms automate the verification of medical expenses—ranging from doctor co-pays and prescription drugs to specialized equipment like crutches or blood pressure monitors—ensuring that the tax-free status of the plan is never jeopardized.
Conclusion
As the 2026 tax year approaches, the choice between HRAs and health stipends will likely be dictated by an organization’s size, its internal administrative capacity, and its financial objectives. HRAs offer a sophisticated, tax-efficient mechanism for delivering health benefits that satisfy federal mandates and provide significant savings for both the company and the worker. Health stipends, while less efficient from a tax perspective, offer a simplicity that may appeal to micro-businesses or those seeking to provide additional "perks" beyond a standard health plan.
Ultimately, the transition from traditional group plans to these personalized reimbursement models represents a maturation of the American healthcare system. By decoupling health insurance from a specific employer-selected carrier and moving toward a defined-contribution model, organizations are empowering their workforce to become more informed consumers of healthcare, while simultaneously stabilizing their own long-term financial health. Organizations considering these options should consult with benefits specialists to ensure their plan design meets the rigorous standards of the IRS and the Department of Labor.