As the fiscal landscape of 2026 presents ongoing challenges for American businesses, the cost of providing competitive employee benefits has reached a critical juncture. Traditional group health insurance, long the standard for corporate America, continues to see premium increases that often outpace inflation, leaving small to mid-sized enterprises (SMEs) and nonprofit organizations in a difficult position. To maintain talent retention without compromising financial stability, an increasing number of organizations are pivoting toward Health Reimbursement Arrangements (HRAs). These employer-funded, tax-advantaged models represent a shift from "defined benefit" healthcare to a "defined contribution" strategy, offering a level of flexibility and cost-predictability that traditional plans often lack.
The Strategic Shift in Employee Healthcare Benefits
An HRA is not an insurance policy in itself but a formal, employer-funded health benefit that reimburses employees for out-of-pocket medical expenses and, in many cases, individual health insurance premiums. Unlike traditional group plans, where the employer selects a "one-size-fits-all" policy for the entire workforce, an HRA allows the employer to set a fixed monthly allowance. Employees then utilize these funds to procure the medical services or insurance plans that best align with their personal health needs and family circumstances.
The adoption of HRAs has surged as businesses seek to mitigate the risks associated with volatile insurance markets. By utilizing an HRA, the employer’s liability is capped at the total allowance offered, and funds are only disbursed when an employee incurs a qualified expense. This "unfunded notional account" structure ensures that unused funds remain with the employer at the end of the plan year, providing a significant budgetary advantage over the "pay-per-head" model of traditional group insurance.
A Chronology of HRA Evolution and Regulatory Milestones
The current diversity of HRA options is the result of over two decades of regulatory evolution aimed at expanding healthcare access and portability.
- 2002: The Internal Revenue Service (IRS) formally recognized HRAs, allowing employers to reimburse employees for medical expenses on a tax-free basis, provided the employer maintained full control over the funds.
- 2010: The passage of the Affordable Care Act (ACA) introduced new "market reforms," which initially restricted the use of "stand-alone" HRAs that were not integrated with a group health plan.
- 2016: Congress passed the 21st Century Cures Act, which established the Qualified Small Employer Health Reimbursement Arrangement (QSEHRA). This allowed businesses with fewer than 50 employees to offer a stand-alone HRA for the first time since the ACA’s implementation.
- 2020: Federal agencies finalized rules creating the Individual Coverage HRA (ICHRA) and the Excepted Benefit HRA (EBHRA), significantly expanding the ability of employers of all sizes to move away from traditional group plans.
- 2024–2026: Continued adjustments to contribution limits and the refinement of "employee classes" have solidified HRAs as a mainstream alternative to the traditional Blue Cross/Blue Shield or UnitedHealthcare group models.
Detailed Analysis of HRA Variants in 2026
To navigate the 2026 benefits landscape, employers must distinguish between the six primary types of HRAs currently recognized by the IRS and the Department of Labor.
1. Individual Coverage HRA (ICHRA)
The ICHRA is arguably the most versatile HRA available today. Available to organizations of any size, it has no government-mandated contribution limits. Its primary innovation is the use of "employee classes." Employers can divide their workforce into 11 distinct categories—such as full-time, part-time, seasonal, or geographic location—and offer different allowance amounts to each. This allows a firm to offer more robust support to senior staff or those in high-cost-of-living areas while maintaining a basic benefit for other groups.
2. Qualified Small Employer HRA (QSEHRA)
Designed specifically for small businesses with fewer than 50 full-time equivalent (FTE) employees, the QSEHRA is a "stand-alone" benefit. For the 2026 plan year, the IRS has set annual contribution limits at $6,450 for self-only coverage and $13,100 for family coverage. The QSEHRA requires that the employer does not offer any other group health plan, ensuring that the HRA is the primary vehicle for healthcare support.
3. Group Coverage HRA (GCHRA)
Also known as an "Integrated HRA," the GCHRA works alongside a traditional group health insurance plan. It is often used to offset the high deductibles associated with modern group policies. For example, an employer might choose a lower-premium High Deductible Health Plan (HDHP) and then use a GCHRA to reimburse employees for the first $2,000 of their deductible, effectively creating a "custom" insurance tier.
4. Excepted Benefit HRA (EBHRA)
The EBHRA is intended for "excepted benefits" rather than primary medical insurance. This includes dental, vision, and long-term care. For 2026, the annual contribution limit is $2,200. This is a strategic tool for employers who provide a standard group medical plan but want to offer additional, flexible funds for specialized care without increasing the complexity of the main insurance policy.
5. Retiree HRA and Dental/Vision HRA
The Retiree HRA allows firms to provide ongoing healthcare support to former employees, often serving as a tax-efficient alternative to traditional pension-linked healthcare. The Dental/Vision HRA is a more restricted version of the EBHRA, specifically targeted at ancillary care, often paired with Health Savings Accounts (HSAs) to maintain compliance with "HSA-qualified" high-deductible plans.

Supporting Data: The Economic Case for HRAs
Current market data suggests that the "Defined Contribution" healthcare model is gaining significant traction. According to industry reports, the number of employees covered by an ICHRA has grown by approximately 25% annually since 2022.
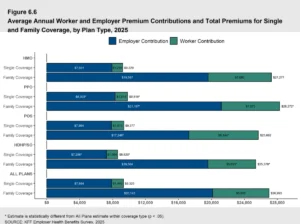
The primary driver is cost-control. In a traditional group plan, an employer might face a 15% premium hike year-over-year due to a single "high-claim" individual in their small risk pool. Conversely, with an HRA, the employer’s cost is fixed. If the cost of individual insurance premiums rises, the employee may need to choose a different plan or pay the difference, but the employer’s budget remains predictable.
Furthermore, HRAs offer significant tax advantages. Contributions are 100% tax-deductible for the employer and are not subject to payroll taxes (FICA/FUTA). For the employee, reimbursements are generally free from federal and state income taxes, provided they maintain "Minimum Essential Coverage" (MEC).
HRA vs. HSA: A Critical Distinction
A common point of confusion in human resources is the difference between an HRA and a Health Savings Account (HSA). While both offer tax advantages, their structures are fundamentally different:
- Ownership: The employer owns the HRA. If an employee resigns, the funds remain with the company. The employee owns the HSA; the account is portable and stays with the individual regardless of their employment status.
- Funding: Only employers can fund an HRA. Both employers and employees can contribute to an HSA.
- Availability: HRAs can be offered with various types of insurance (or none, in the case of stand-alone HRAs). HSAs must be paired with an IRS-qualified High Deductible Health Plan (HDHP).
Official Responses and Industry Implications
Policy analysts from organizations like the Society for Human Resource Management (SHRM) have noted that the rise of HRAs reflects a broader trend toward the "personalization" of the workplace. "Employees in 2026 value choice and portability," notes one benefits consultant. "An HRA allows a 25-year-old single employee to choose a plan with high fitness benefits, while a 50-year-old employee with a family can choose a plan with robust pediatric and chronic care coverage, all using the same employer allowance."
However, the shift is not without critics. Some labor advocates argue that moving away from group plans places more "plan-shopping" burden on the employee. To counter this, many HRA administrators have developed sophisticated digital marketplaces that allow employees to compare individual plans and enroll directly through their benefits dashboard.
Compliance and Administration Requirements
Operating an HRA requires strict adherence to IRS and Department of Labor (DOL) regulations. Key requirements include:
- Plan Documents: Employers must have a formal, written plan document that outlines eligibility, allowance amounts, and types of reimbursable expenses.
- COBRA Compliance: Most HRAs (except for some small-employer versions) are subject to COBRA, meaning employers must offer a "run-out" period or continuation of the benefit upon an employee’s departure.
- HIPAA Privacy: Because employers are technically handling "Protected Health Information" (PHI) during the reimbursement process, they must ensure strict data security. This is the primary reason the majority of firms utilize third-party HRA administrators to handle claim reviews and verification.
Conclusion: The Future of the Employer-Employee Healthcare Contract
As we move through 2026, the Health Reimbursement Arrangement is no longer a niche "alternative" but a cornerstone of modern benefits strategy. By decoupling the funding of healthcare from the selection of the insurance plan, HRAs provide a "middle ground" that respects the employer’s budget while honoring the employee’s need for individualized care.
For small businesses and nonprofits, in particular, the HRA represents a democratization of benefits, allowing them to compete with Fortune 500 companies for talent without the prohibitive costs of large-scale group health contracts. As the individual insurance market continues to mature and offer more competitive rates, the logic for HRA adoption only becomes more compelling, signaling a long-term shift in how American workers access and pay for medical care.